language
Cox® Technic Case Report of the Month – www.coxtechnic.com ‐ sent July 2024
Neck Pain with Left Shoulder and Arm Pain Into The Fingers Eased with Cox Technic
by Niko Kalogeropoulos DC, Athens, Greece submitted on 6/12/24
CHIEF COMPLAINT:
This 48‐year‐old female, mother of two teenagers and self‐employed pharmacist, presented with severe cervical pain, radiating to left shoulder and left lateral elbow with pain and numbness into the left thumb, index, and tip of middle finger.

HISTORY:
She has been treated in the past for similar history/complaints of cervical spine pain and radiation to right arm and hand. Due to distance, she has not maintained a treatment plan until symptoms arise. This episode began two days prior to the first visit following coughing and housework with excruciating, stabbing pain in the cervical spine with radiation down the left arm unlike prior episodes of right‐sided pain and symptomatology. She reported the pain as a 10 on the VAS, 0‐10 where zero is no pain. She is unable to sleep or rotate her head which prevents her from driving. She was driven to the clinic for her first visit.
EXAMINATION:
Range of motion: 25 degrees if left cervical rotation and 35 degrees right, hindered hindered by pain. Left rotation produced pain down the left arm. Cervical flexion was 25 degrees, and extension was about 5 ‐10 degrees. Myotomes were +4 mainly due to pain inhibition. Reflexes were +2. Dermatomes with pinwheel revealed hypesthesia over the index finger and tip of middle finger and thumb. All other vitals were normal. No abnormalities with other systems were detected. She showed some signs of distress and exhaustion from lack of sleep.
DIAGNOSTIC IMAGING FINDINGS:
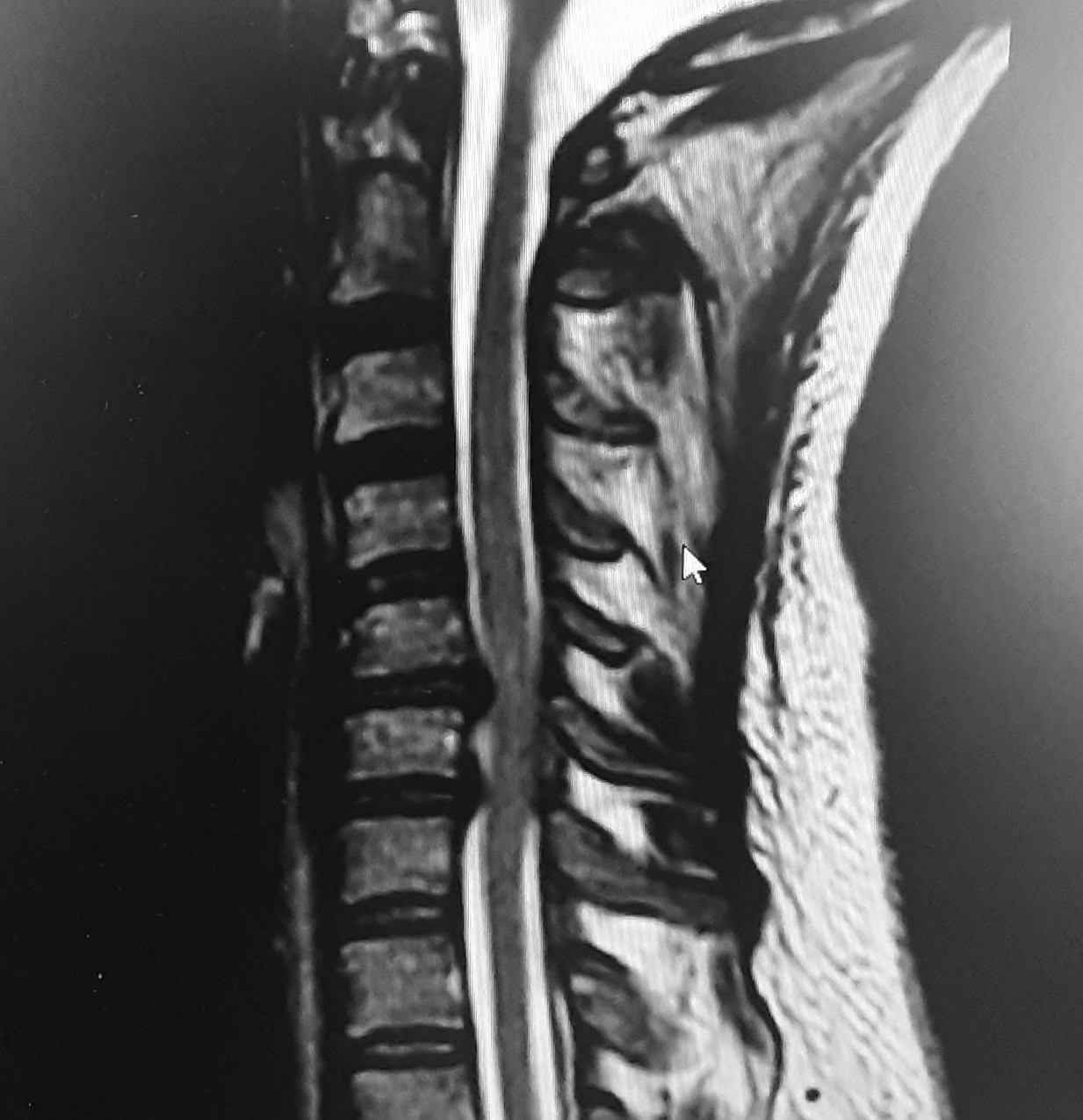
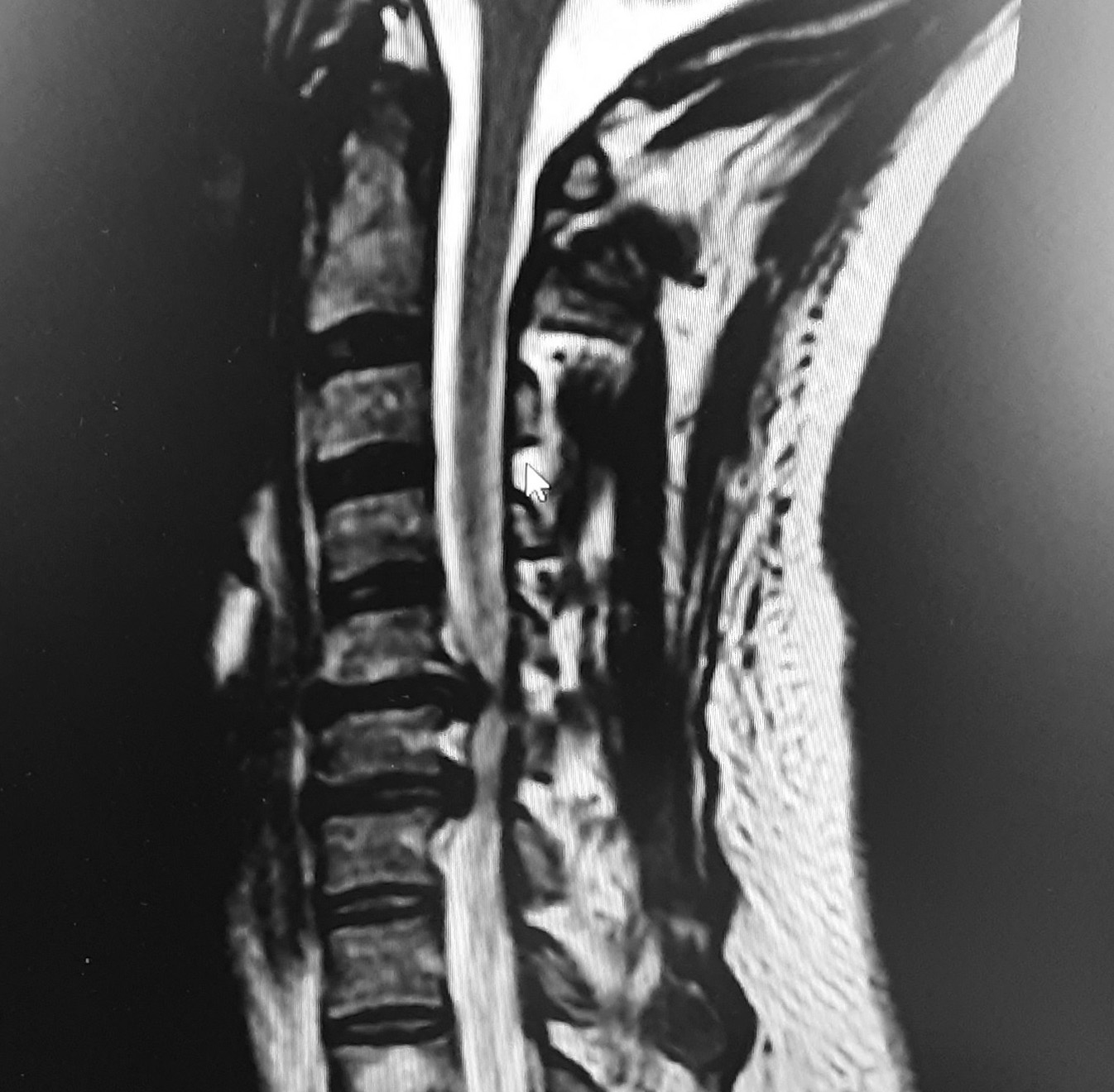
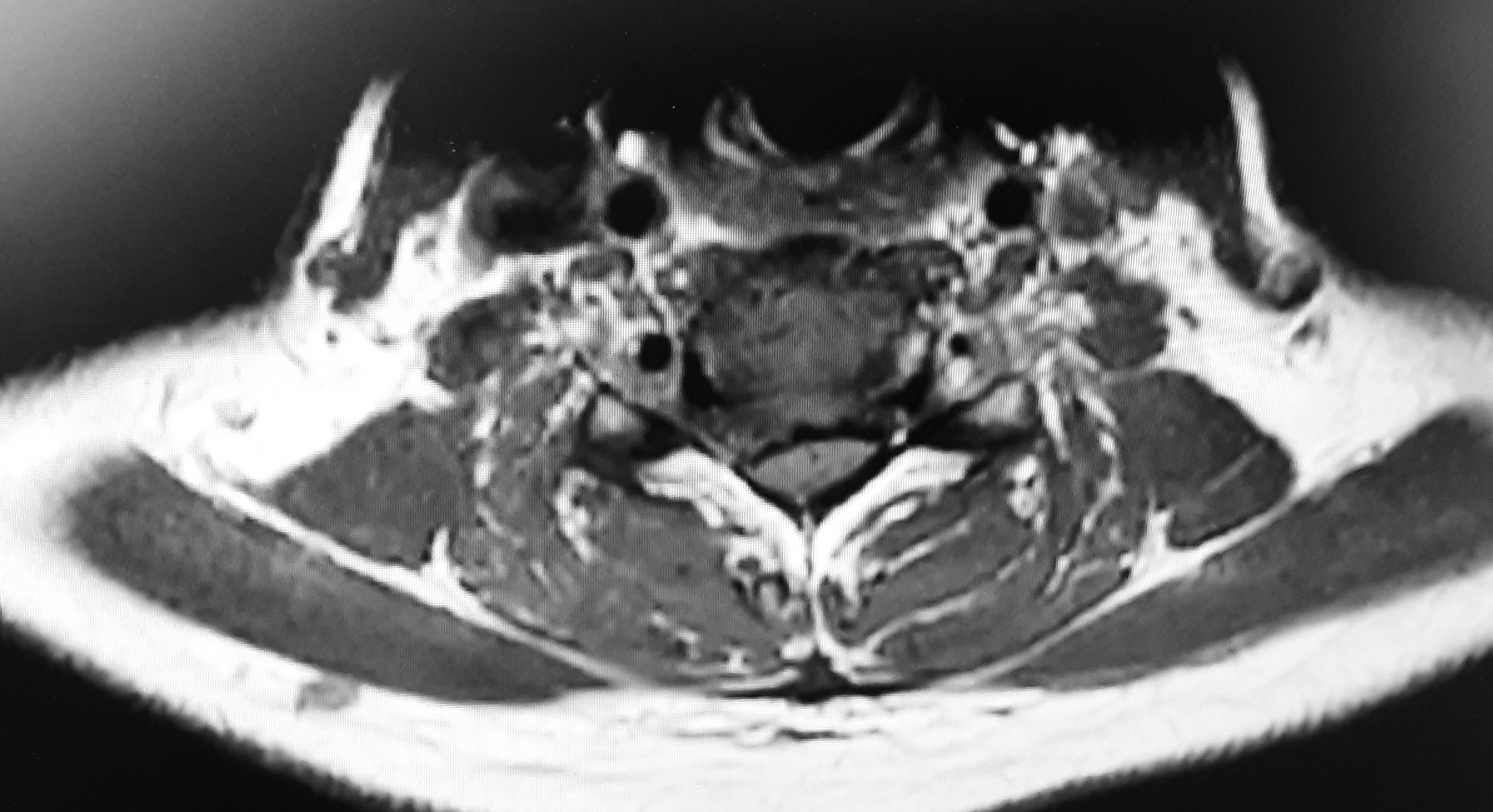
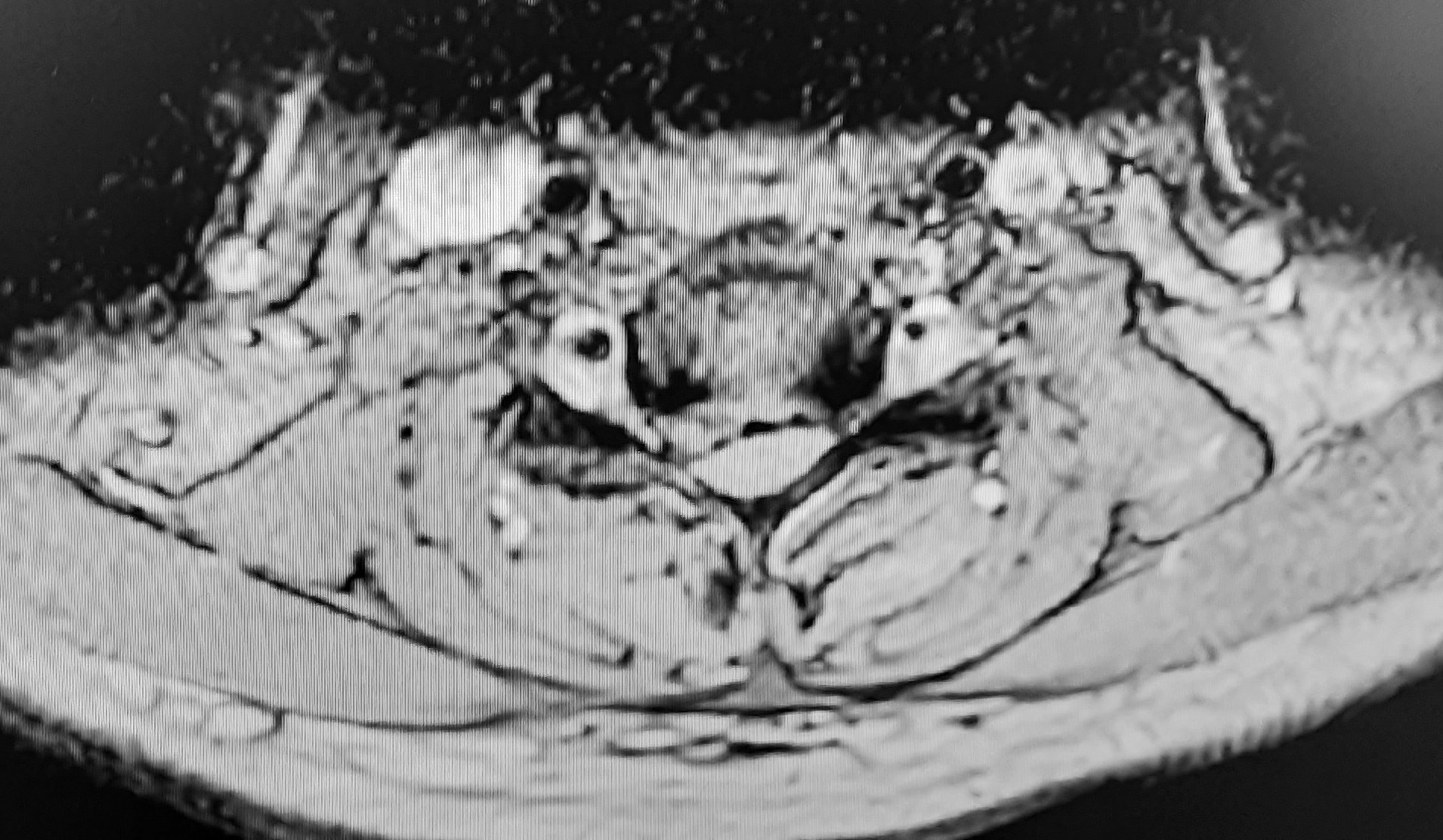
Alordosis with gibbus formation noted at the C5‐C6 level. Advanced degenerative disc disease is visible at C5 and C6 levels with intervertebral disc extrusion applying severe compressive pressure on the spinal cord showing Kang changes (Figures 1 and 2). Figure 3 is a T2 axial cut showing right disc herniation that contacts and displaces the spinal cord. Figure 4 shows the right sided foraminal and lateral recess stenosis due to disc herniation clearly. Notably, the spinal canal is under compression, particularly the right foraminal canal which is severely to totally closed: yet, not right cervical spine or extremity pain is present, only left C6 dermatome pain.
CASE DIAGNOSIS:
Degenerative disc disease and disc extrusion with compressive forces on the spinal canal and nerve roots of the C5‐C6 and C6‐C7 spinal levels, affecting the C6 spinal nerve root mainly.
TREATMENT AND FOLLOW UP:
The patient was instructed in the initial visit that her case was a difficult one and that she needed to consult a neurosurgeon if progressive neurological signs evolved or if the pain became unbearable especially within 6‐8 visits 50% relief was not achieved (1,2).
Treatment consisted of long Y‐axis distraction using the Cox®8 Table’s cervical head piece, more specifically the occiput pump, and C4 arch contact. Adjustments were performed in the upper cervical spine, C1 and C2 mainly, and then when 50 % of the pain subsided, C3 and T2 and T3 areas were also treated. (3) Myofascial trigger points and functional range release of the left infraspinatus muscle was performed. The infraspinatus referred pain and numbness extending to the index finger. Ice to cervical area and infraspinatus muscle and glucosamine sulphate with chondroitin sulphate were recommended for home. As a pharmacist, the patient refused to take the suggested supplementation.
TREATMENT OUTCOMES:
The treatment regime consisted of progressive and rapid relief of the symptoms.
In summary, 8 treatments over one month were administered. Treatments are continuing at one every 10 days, and a maintenance program will be initiated.
DISCUSSION WITH CITATION REFERENCES:
Similar outcomes have been published regarding Cox® Technic management of disc herniations. One case of a moderate‐sized left posterolateral disc herniation at C6/C7 causing severe foraminal stenosis reported relief in 15 treatments in 10 weeks with a 2‐year follow‐up reporting stable subjective and objective findings. (4) Another case regarding a C6/C7 left posteromedial disc noted relief of neck and arm pain in 10 treatments in 4 weeks with continued relief at 8 months (5).
REFERENCES:
Cox JM: Low Back Pain: Mechanism, Diagnosis, Treatment 7th ed. Philadelphia: Lippincott Williams and Wilkins, 2011, pages 445‐515
Cox JM: Neck, Shoulder and Arm Pain: Mechanism, Diagnosis, Treatment. 4th ed. Fort Wayne IN: Cox Technic Resource Center Inc, 2014, pages 105‐106
Cox JM: Neck, Shoulder and Arm Pain: Mechanism, Diagnosis, Treatment. 4th ed. Fort Wayne IN: Cox Technic Resource Center Inc, 2014, pages 74, 95‐96
Gudavalli S, Kruse R: Foraminal stenosis with radiculopathy from a cervical disc herniation in a 33‐year‐old man treated with flexion‐distraction decompression manipulation. Journal of Manipulative and Physiological Ther apeutics 2008; 31(5):376‐380
Cox® Technic Case Report of the Month – www.coxtechnic.com ‐ sent July 2024
| Cookie | Duration | Description |
|---|---|---|
| cookielawinfo-checkbox-analytics | 11 months | This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics". |
| cookielawinfo-checkbox-functional | 11 months | The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional". |
| cookielawinfo-checkbox-necessary | 11 months | This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary". |
| cookielawinfo-checkbox-others | 11 months | This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other. |
| cookielawinfo-checkbox-performance | 11 months | This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance". |
| viewed_cookie_policy | 11 months | The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data. |