Cox® Technic Case Report of the Month – www.coxtechnic.com ‐ sent July 2024
Lower Back Pain Radiating Down on the Left Leg
by Niko Kalogeropoulos DC
A 39 y.o. male patient presented to my clinic a year ago complaining of lower back pain radiating down the left posterior lateral thigh into the left posterior lateral calf and lateral aspect of the foot. Numbness and tingling was also present. Walking with the family would be from park bench to park bench, with longer periods of rest than actual walking! Besides the pain and numbness in the leg the hamstring muscles were tight and pulling when he was upright Nights were difficult with pain interrupting sleep, seated was impossible without being forward flexed resting on thighs. Coughing, sneezing and getting out of a chair increased leg pain. Five months prior to his visit he had fallen off his motorbike, injuring his right shoulder.
He was brought in by his father as he could not drive. There was distress on his face. A slight anterior antalgia and a short gait.

ON EXAMINATION:
B SI joints and lumbar fixations, forward flexion was about 40 degrees when pain in LB and leg began. Left leg was short, Left Straight Leg Raise caused pain at about 30 degrees, Myotomes and reflexes revealed no abnormalities.
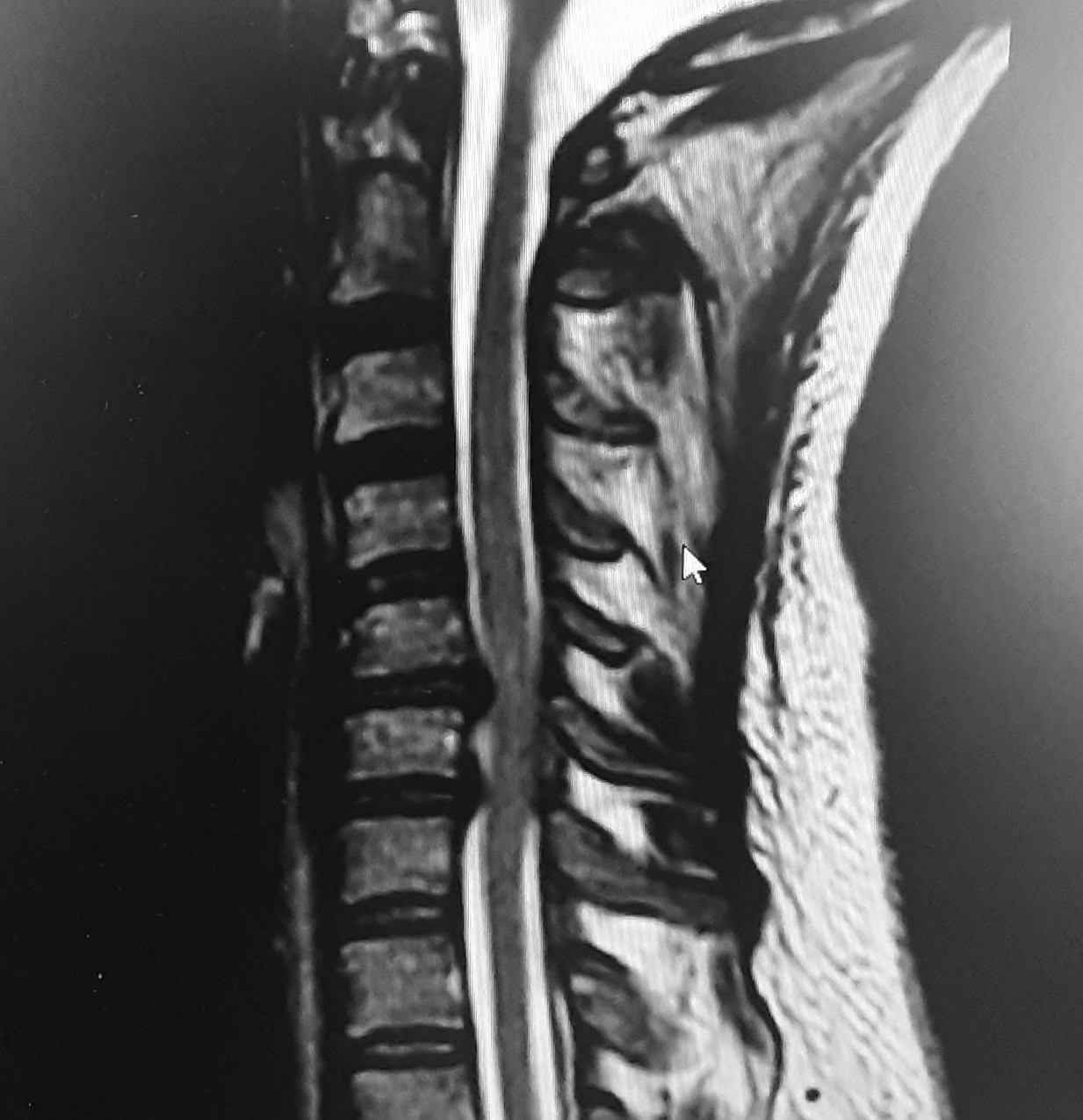
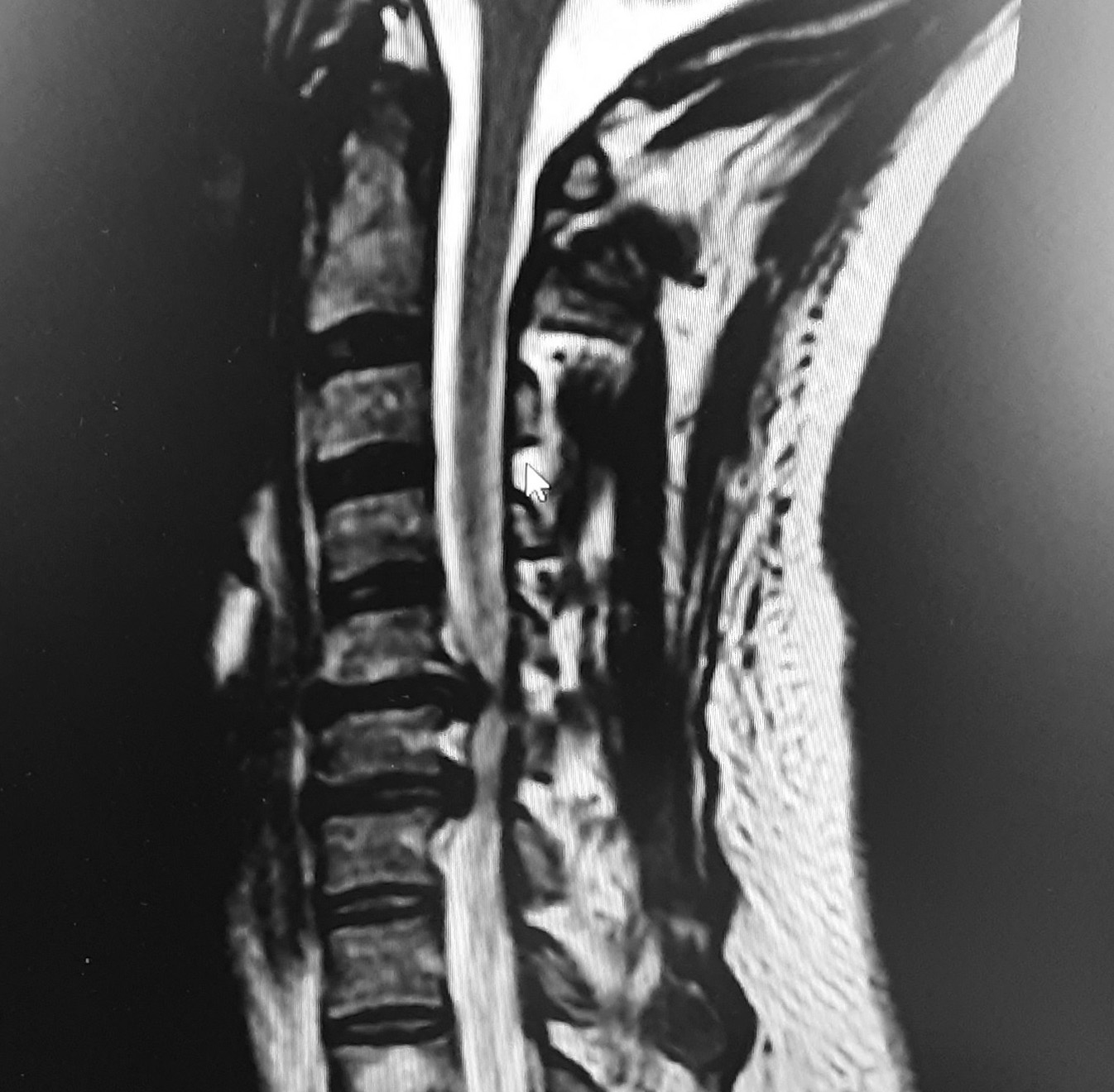
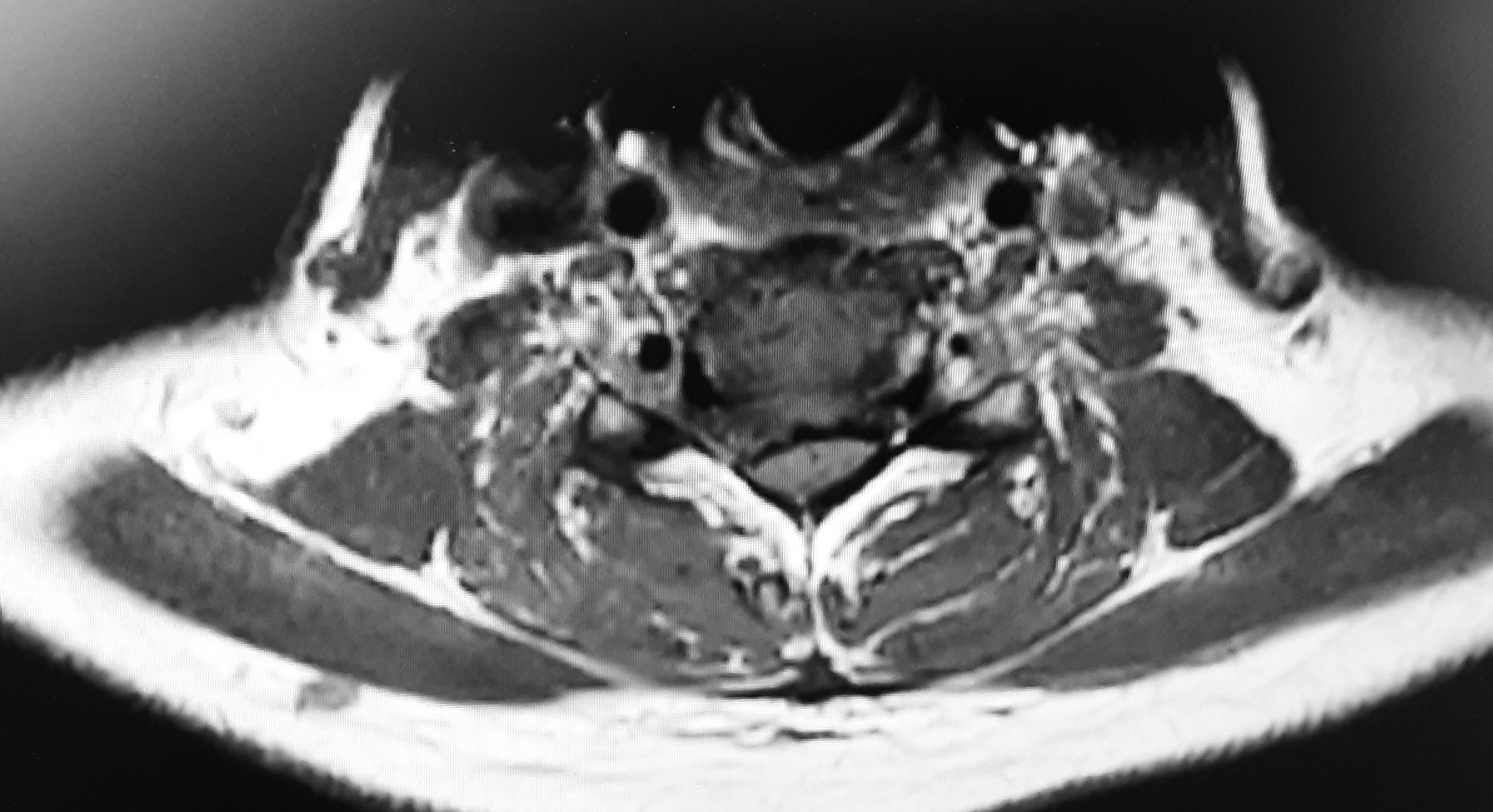
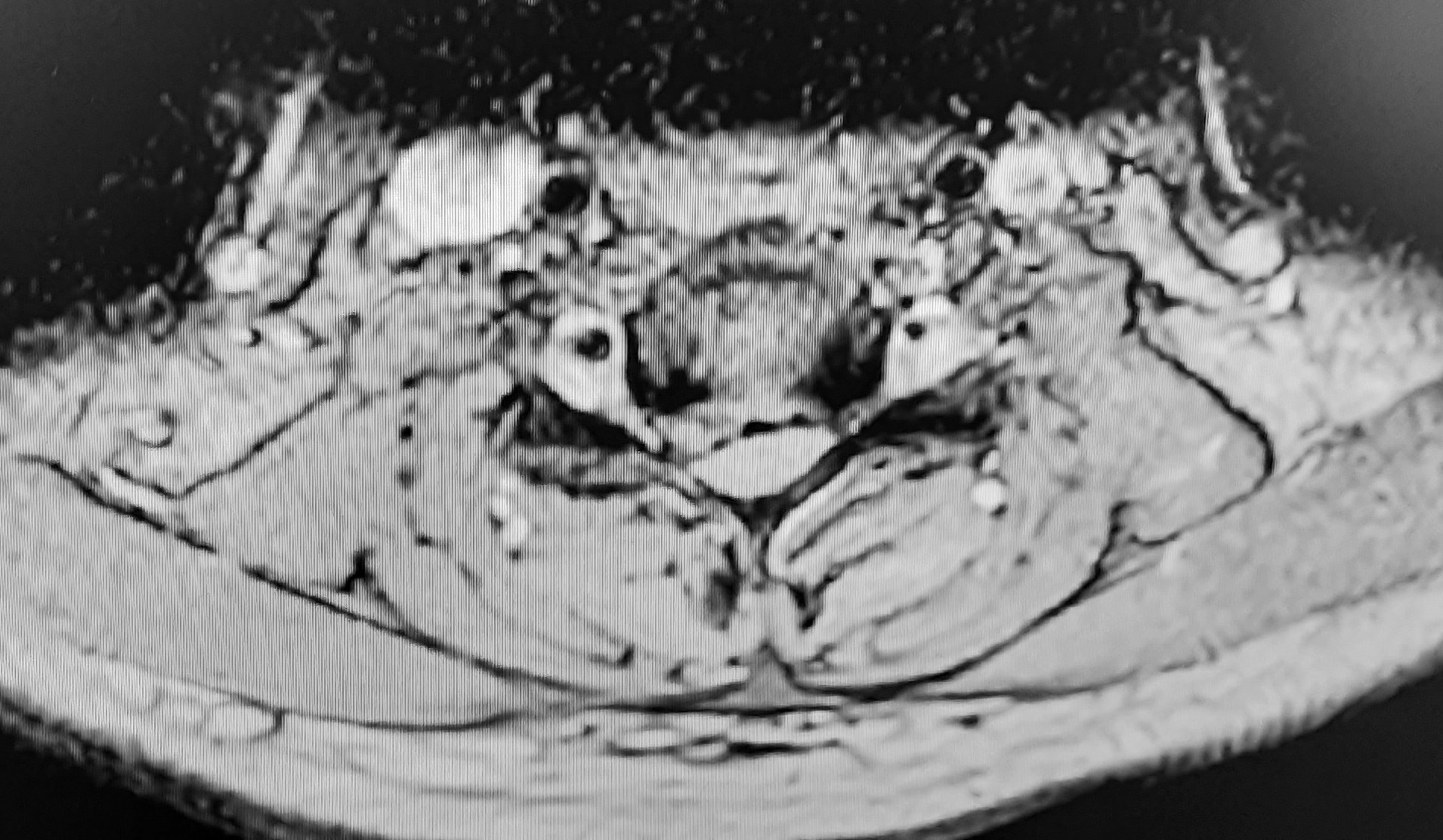
IMAGING:
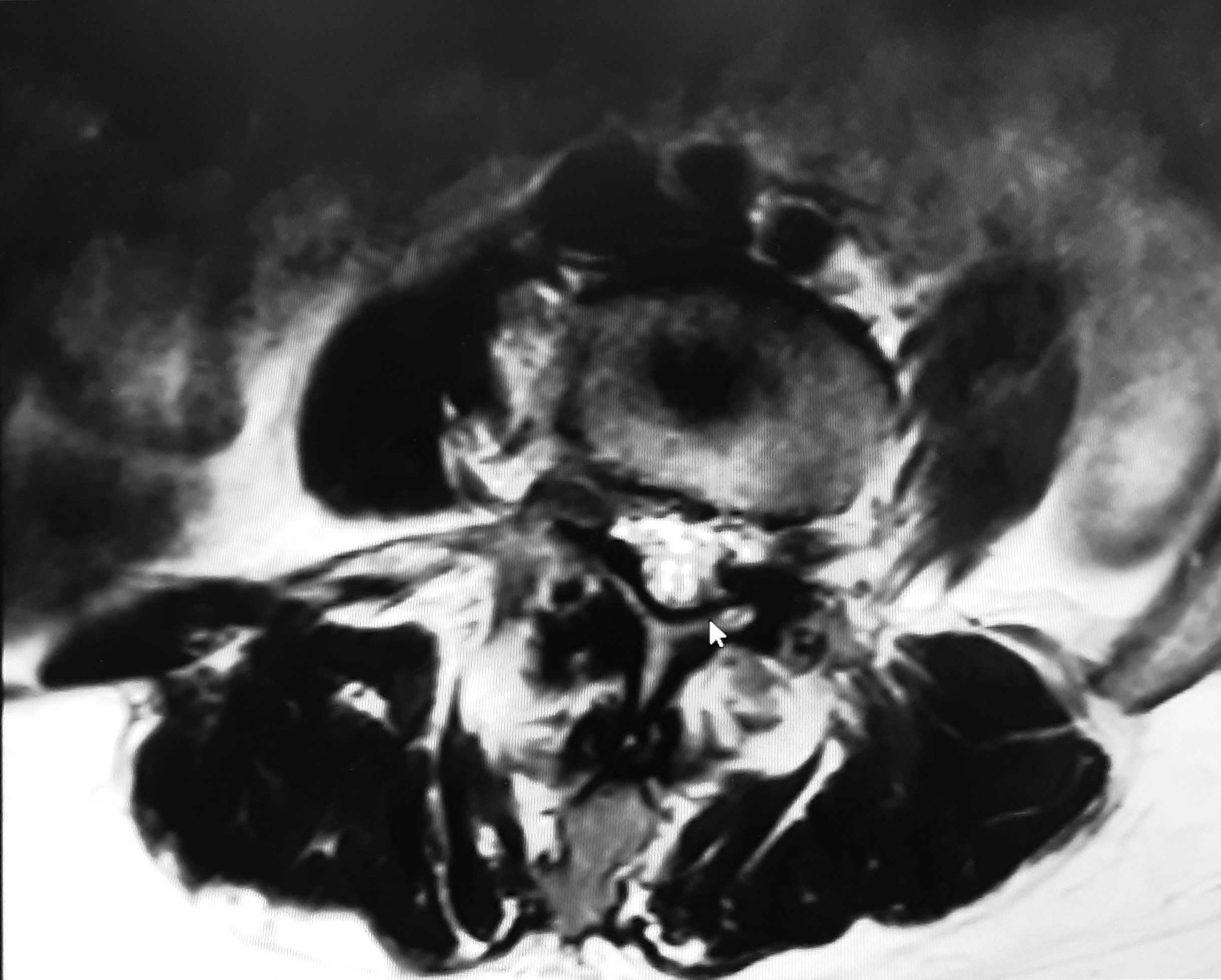
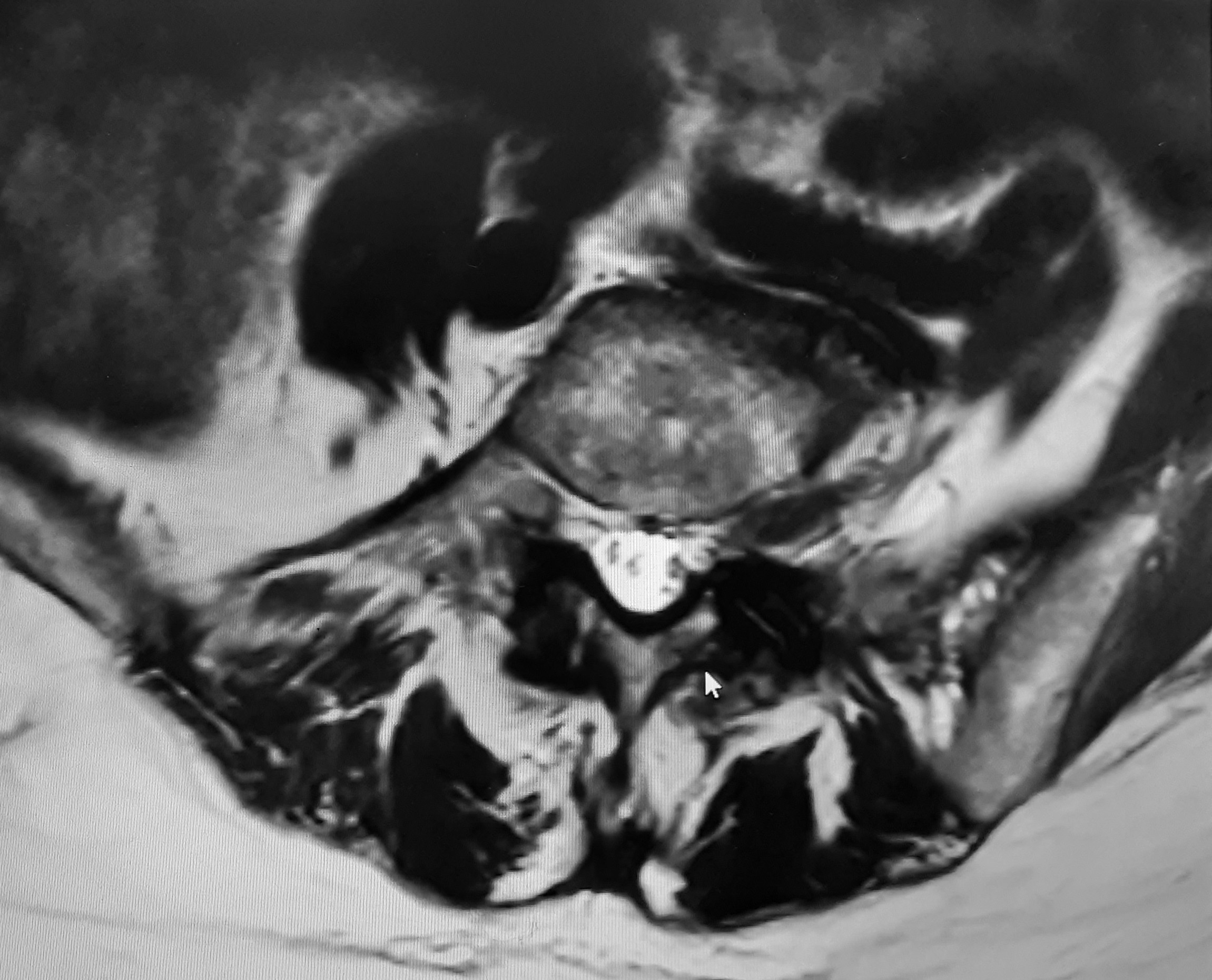
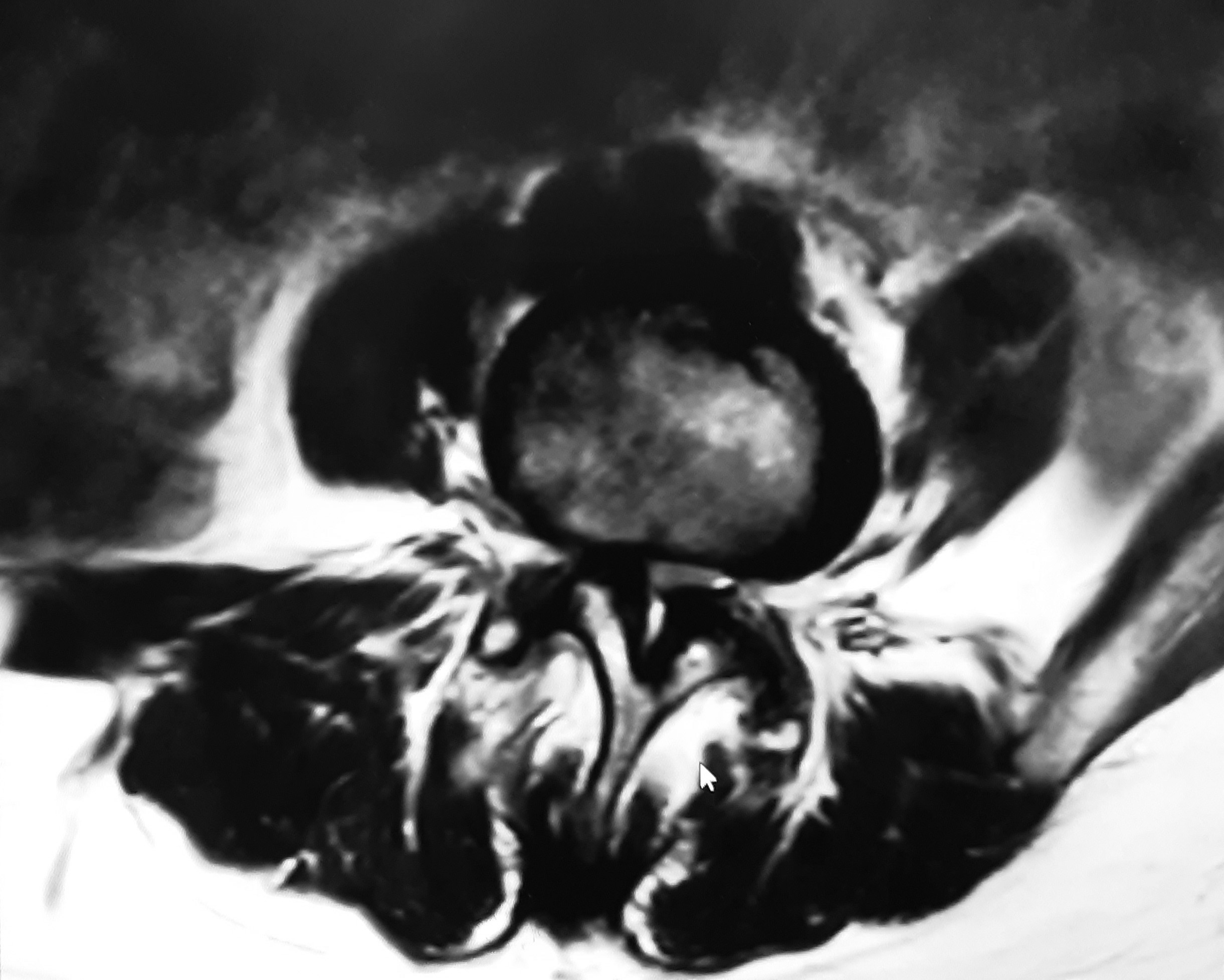
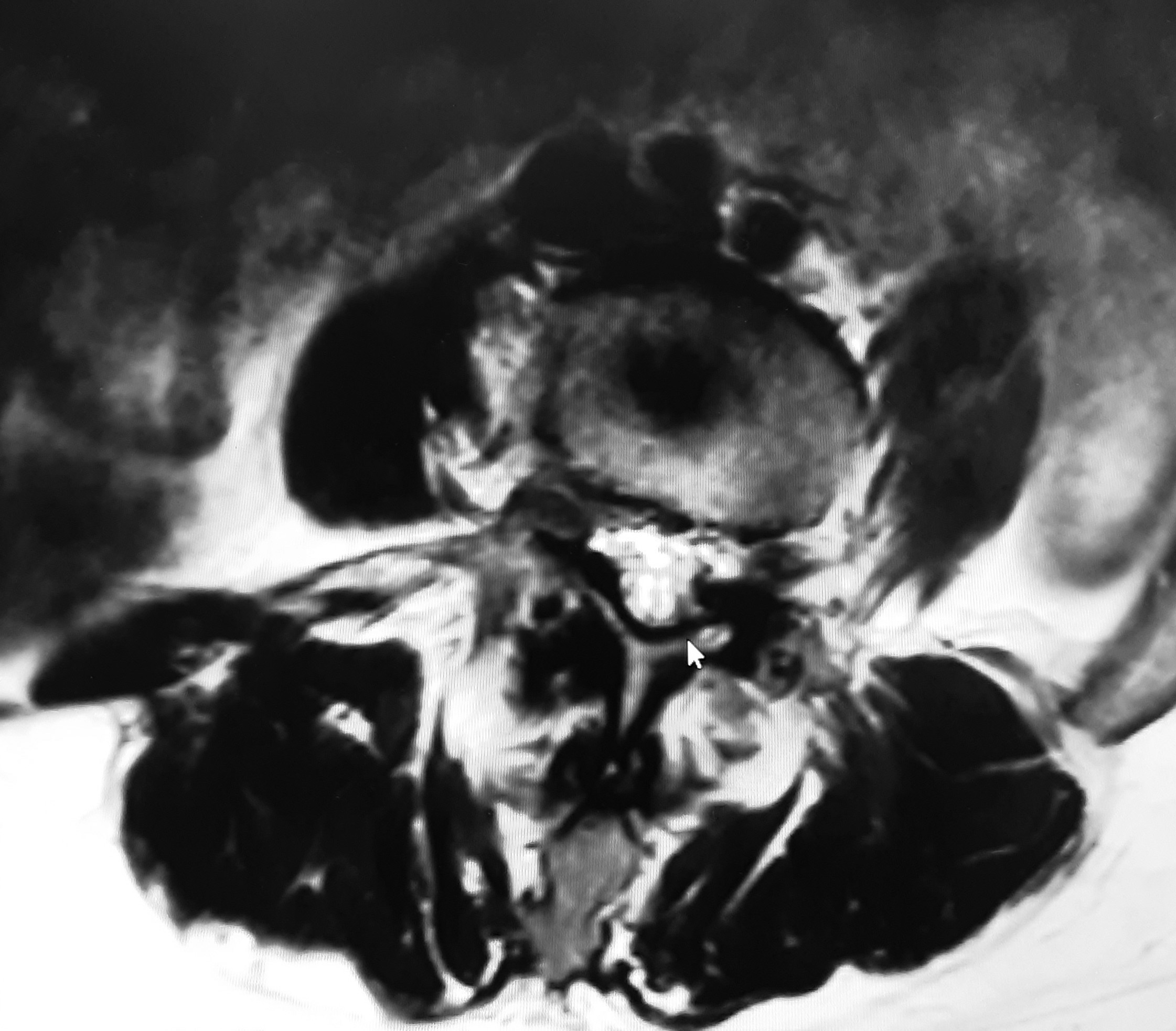
The below images show the Degenerative Disc at L4 and L5 discs, with a buldge at L4 with inflammation, and L5 a large central to left extrusion. Endplate degradation.

figure 1

figure 2
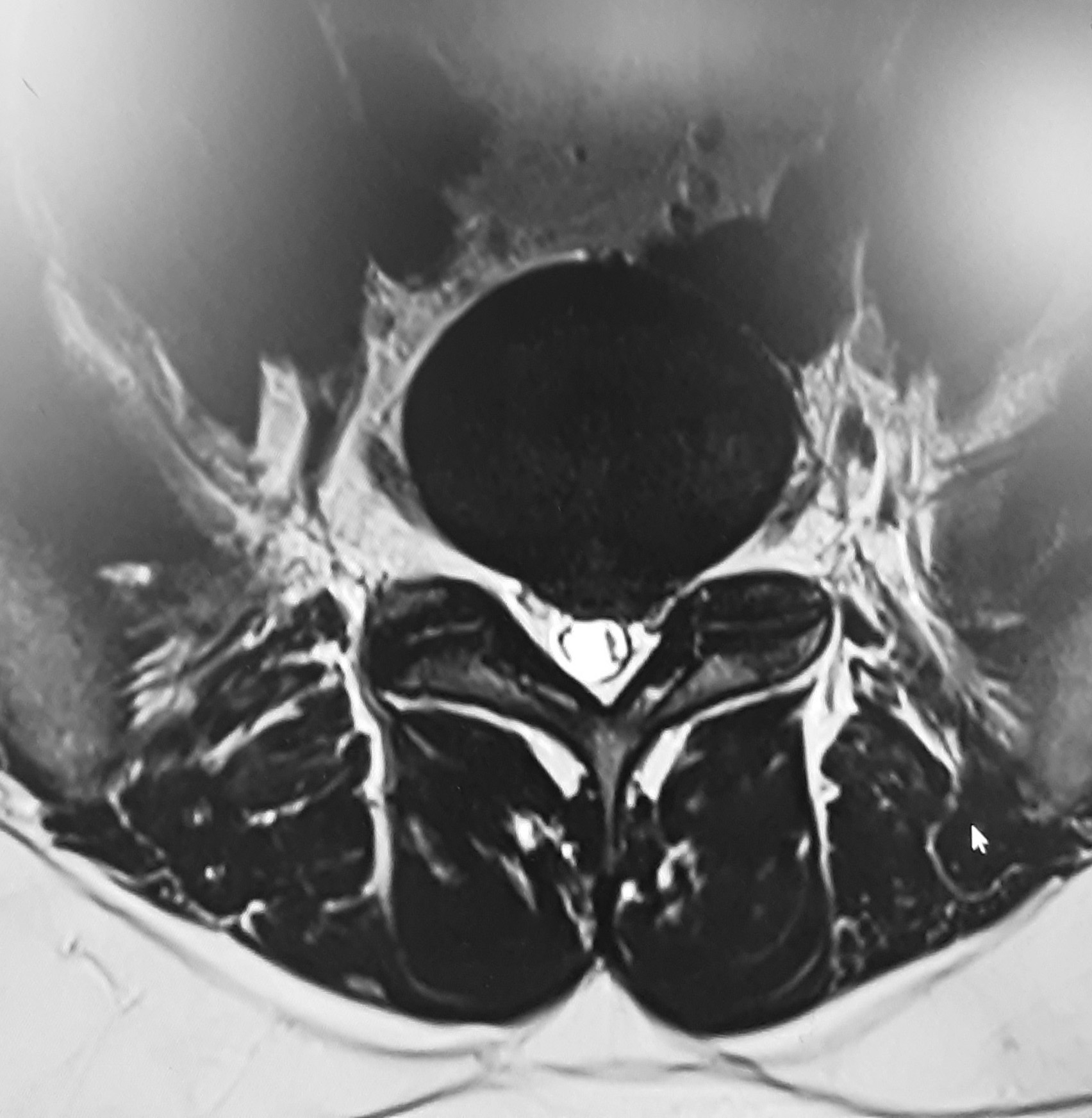
figure 3
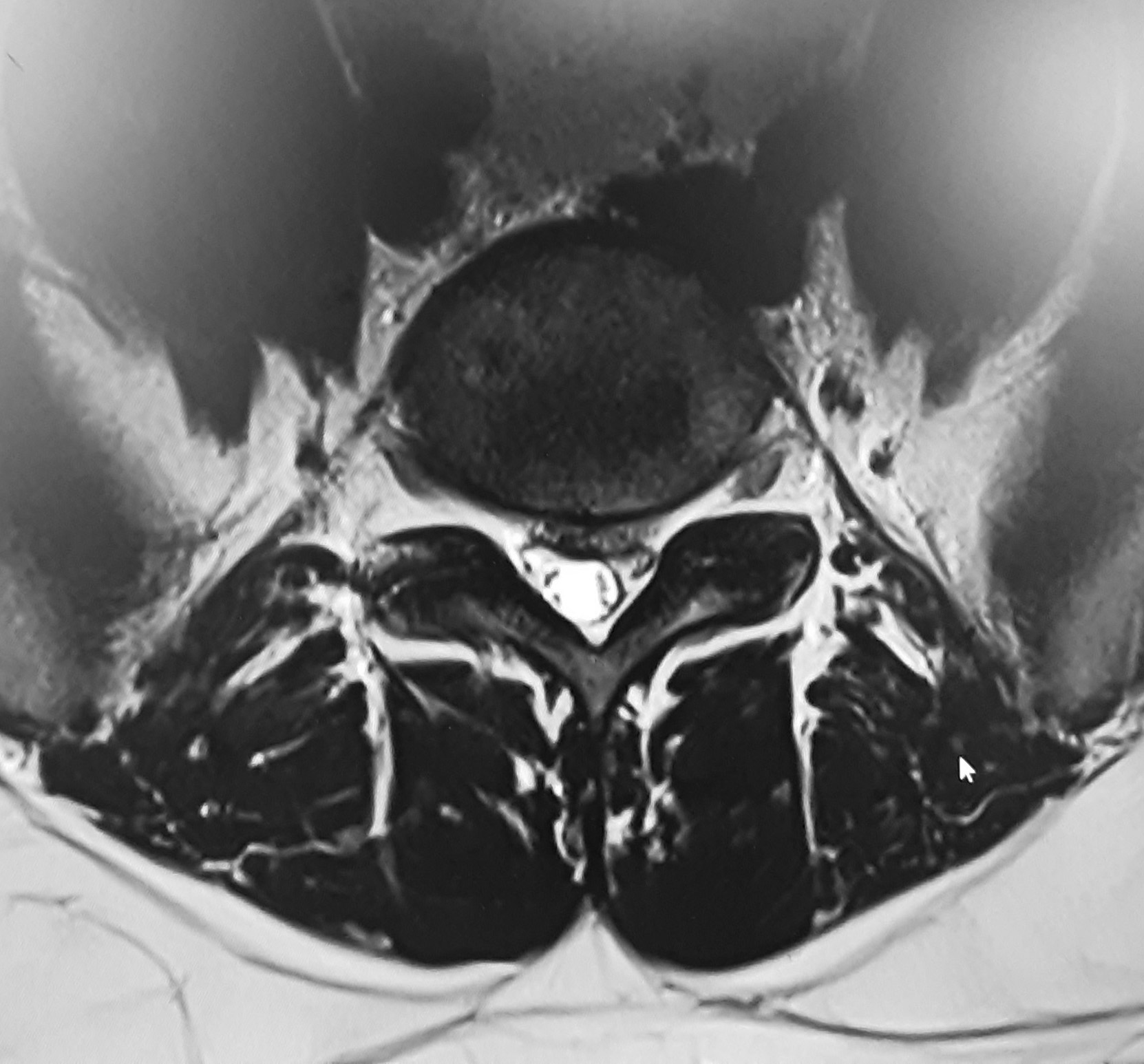
figure 4
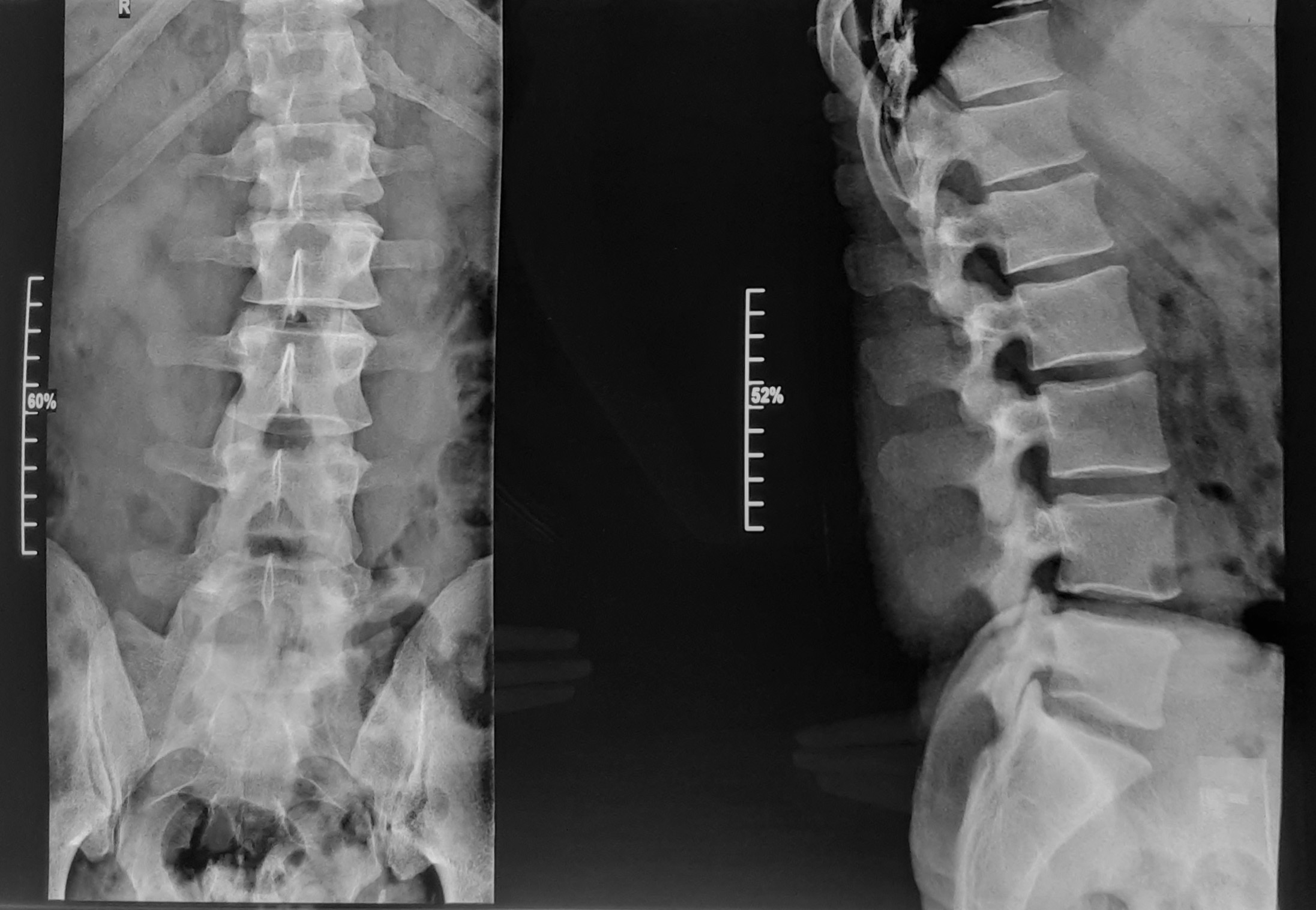
figure 5
This x-ray shows the S1 superior facet encroaching in the IVF.
WORKING DIAGNOSIS:
Stage 3 disc pathology with accompanied disc extrusions and joint fixations.
TREATMENT PLAN:
Treatment was initiated. All treatments consisted of Cox® Technic FlexionDistraction Decompression. First, Protocol 1 (3 sets of 5 four- second pumps from the taut point) was delivered after careful tolerance testing revealed no aggravation, to achieve 50% subjective and objective clinical improvement. Then Protocol 2 (full range of motion under distraction: flexion, lateral flexion, circumduction) but mainly long Y‐axis distraction would be implemented starting from L4 and L3. There were also minimal Gonstead Adjustments delivered to the sacrum, pelvis, cervical region and upper thoracics at separate sessions. Trigger points were deactivated in the gluteal medius and minimus on the left as well as piriformis. Treatment sessions were twice a week till 50% improvement was reached thereafter we moved onto once a week. Strengthening core exercises would be shown to do as homework. Correct seated posture advise will be given it at the office or on the bike.
OUTCOME:
The patient had a rapid response to the treatment plan. From the first session felt an improvement, the second he could sleep at night and lumbar range of motion increased with less pain. On the fourth ROM increased further and only had pain in the left gastroc, posterior to the peroneal head. Post fifth session felt ‘better than ever’. A week later we had a relapse where whole leg pain returned. Post one treatment the symptoms subsided quickly and was feeling good. After the nineth treatment the patient was able to do everything, walking with family was not a mission anymore, was able to sit at work and on the motorbike. The nine treatment sessions were done over a three month period. It has been over a year and patient has come in for maintenance care once every two months. Last visit was 19/09/2024 where patient reported that he even plays football and basketball with his son!
DISCUSSION:
The one things that I have learned from Dr. James M. Cox is not to be afraid of these cases, in fact one need to address or encompass them. It is one of many cases that I have seen that proves Dr. Cox’s teachings that these cases can be helped with Cox flexion distraction decompression technic. Incidentally the patient is not doing his strength exercises, although he is working regularly on his posture. One of the important aspects one need to address to maintain the pain free state is strengthening exercises, and unfortunately way to often I hear this is not the case. I believe many of our pains are there to wake us up and for us to make a change but, I’ve noticed that once we are pain free we forget our responsibilities.
Cox® Technic Case Report of the Month – www.coxtechnic.com ‐ sent July 2024